Искусство пальпации остеопата (18)
Леон Чейтоу – Искусство пальпации (18).
Леон Чейтоу – Искусство пальпации (01)
Леон Чейтоу – Искусство пальпации (02)
Леон Чейтоу – Искусство пальпации (03)
Леон Чейтоу – Искусство пальпации (04)
Леон Чейтоу – Искусство пальпации (05)
Леон Чейтоу – Искусство пальпации (06)
Леон Чейтоу – Искусство пальпации (07)
Леон Чейтоу – Искусство пальпации (08)
Леон Чейтоу – Искусство пальпации (09)
Леон Чейтоу – Искусство пальпации (10)
Леон Чейтоу – Искусство пальпации (11)
Леон Чейтоу – Искусство пальпации (12)
Леон Чейтоу – Искусство пальпации (13)
Леон Чейтоу – Искусство пальпации (14)
Леон Чейтоу – Искусство пальпации (15)
Леон Чейтоу – Искусство пальпации (16)
Леон Чейтоу – Искусство пальпации (17)
Леон Чейтоу – Искусство пальпации (18)
Леон Чейтоу – Искусство пальпации (19)
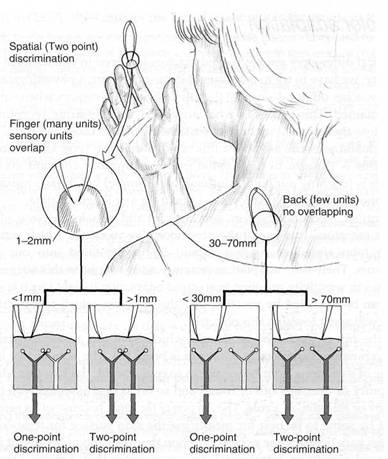
Fig. 2.1 Tactile discrimination. Spatial discrimination: in the two-point test, the spatial discriminative ability of the skin is determined by measuring the minimum separable distance between two tactile point stimuli. The back of the hands, the back and legs rate low (50-100 mm). The fingertips, lips and tongue rate high in this ability (1-3 mm). Intensity discrimination: sensitive areas are also better able to discriminate differences in the intensity of tactile stimuli. Therefore, an indentation of 6 цт on the fingertip is sufficient to extract a sensation. This threshold is 4 times higher in the palm.
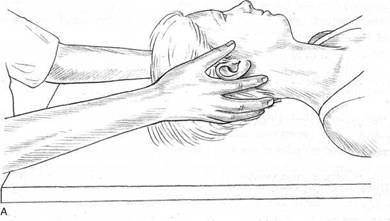
Fig. 2.2A, В Hand position for palpation of cardiovascular activity, inherent motion and other cranial rhythms.
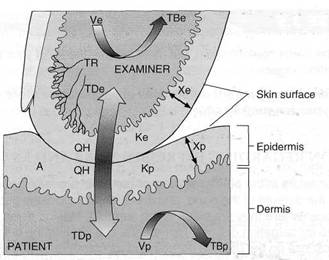
Fig. 3.1 This diagram depicts some of the physical and physiologic factors that affect the thermoreceptor (TR) discharge rate and consequently the temperature sensed in an examiner’s skin in contact with a patient’s skin. The temperature and its rate of change of the examiner’s thermoreceptors are functions of the net effects of the time that the tissues are in contact, their contact area (A), the temperatures (TBe and TBp) and volume flow rates (Ve and Vp) of blood perfusing the examiner’s and patient’s skin, epidermal thickness (Xe and Xp) and thermal conductivity (Ke and Kp) of both, dermal temperature (TDe and TDp) of both, as well of the net heat exchange rate (QH) between the two tissues. QH is strongly affected by the heat transfer properties of material trapped between the two skin surfaces, for example, air, water, oil, grease, hand lotion, dirt, tissue debris, fabric. [Adams et al 1982]
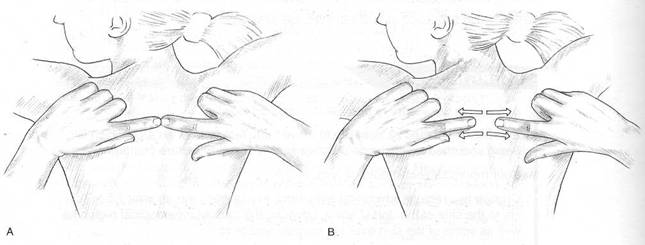
Fig. 3.3(A) Fingers touch each other directly over skin to be tested – very light skin contact only. (B) Pull apart to assess degree of skin elasticity – compare with neighbouring skin area.
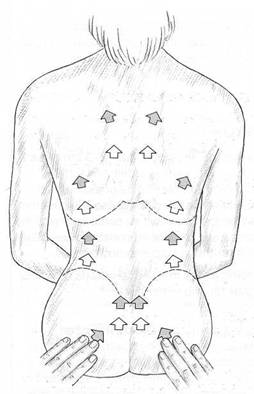
Fig. 3.4 Testing tissue mobility by bilaterally ‘pushing’ skin with fingertip.
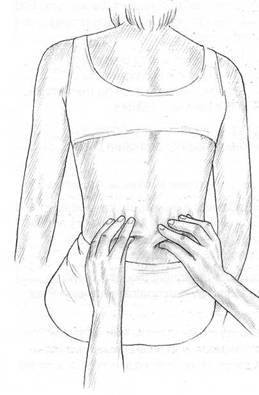 Fig. 3.5 Assessing bilateral elasticity of skin by lifting it in folds.
Fig. 3.5 Assessing bilateral elasticity of skin by lifting it in folds.
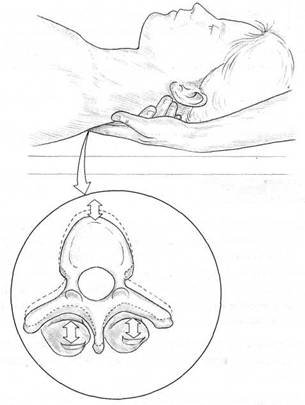
Fig. 4.1 Beal’s ‘springing’assessment for paraspinal facilitation rigidity associated with segmentai facilitation.
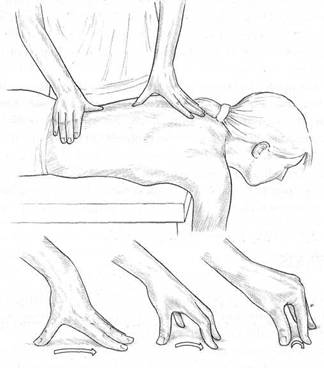
Fig. 4.2 Neuromuscular thumb technique. The operator uses the medial tip (ideally) of the thumb to sequentially ‘meet and match’ tissue density/tension and to insinuate the digit through the tissues seeking local dysfunction.
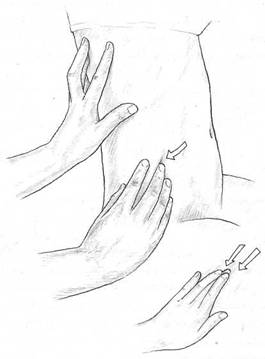
Fig. 4.3 Neuromuscular finger technique. The operator utilises index or middle finger, supported by a neighbouring digit (or two), to palpate and assess the tissues between the ribs for local dysfunction. This contact is used instead of the thumb if it is unable to maintain the required pressure.
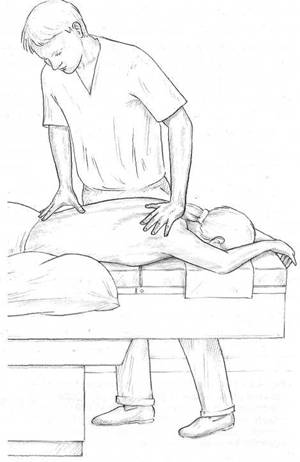
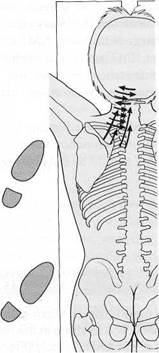
Fig. 4.4 Operator using neuromuscular technique. Note position of feet; straight right arm; right
hand position; thumb position.
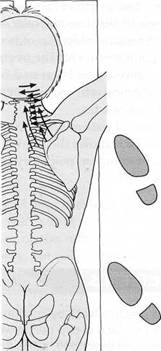
Fig. 4.5A, В Neuromuscular technique. Illustrating position of operator and lines of application.
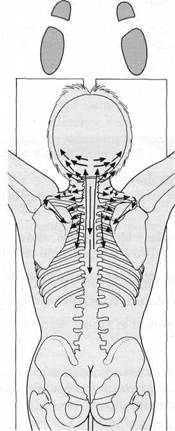
Fig. 4.6 Neuromuscular technique. Illustrating position of operator and lines of application.
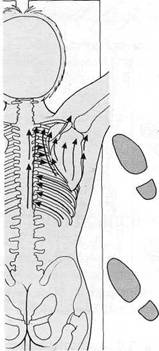
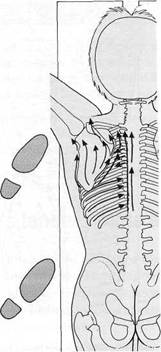
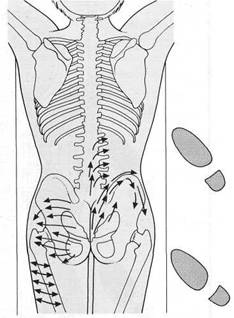
Fig. 4.7A, В Neuromuscular technique. Illustrating position of operator and lines of application.
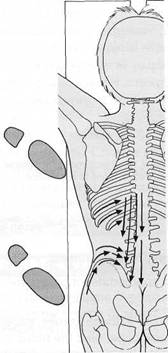
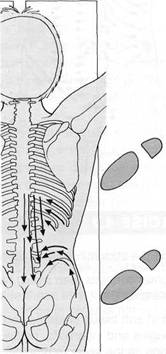
Fig. 4.8A, В Neuromuscular technique. Illustrating position of operator and lines of application.
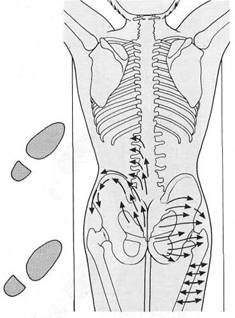
А В
Fig. 4.9A, В Neuromuscular technique. Illustrating position of operator and lines of application.
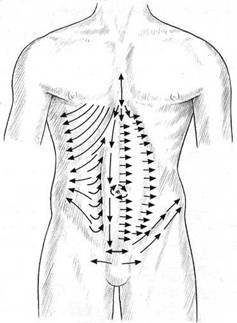
Fig. 4.10 Neuromuscular general abdominal technique. Lines of application.
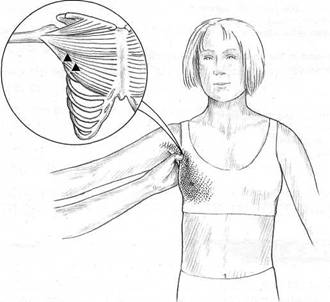
Fig. 4.11 Illustrating trigger points and target area (shaded) in pectoralis major muscle (sternocostai fibres) and ideal palpation method in this area (as well as trapezius, sternomastoid and scalenes).
a) Pincer palpation of trigger points in the sternocostai fibres of the pectoralis major muscle.
b) Referred pain patterns and trigger points (A) in the left pectoralis major muscle. Solid area
shows essential areas of referred pain, and stippled area shows the spillover pain areas. The
lateral free margin of the muscle, which includes fibres of the costal and abdominal sections form
the anterior axillary fold.
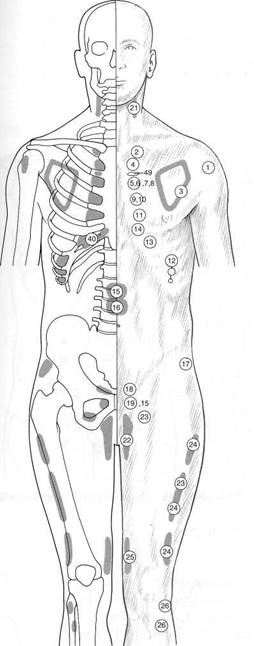
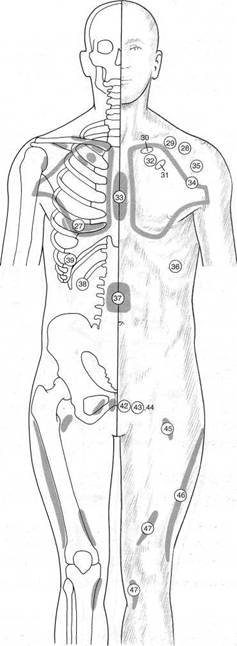
Fig. 4.12 Chapman’s neurolymphatic reflexes.
Fig. 4.13 Chapman’s neurolymphatic reflexes.
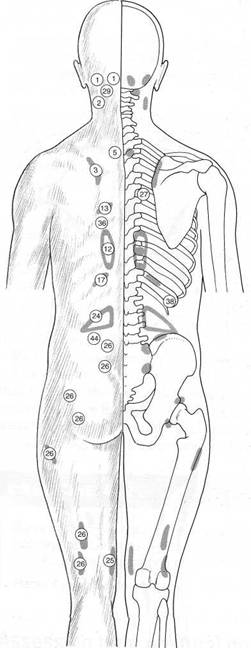
Fig. 4.14 Chapman’s neurolymphatic reflexes.
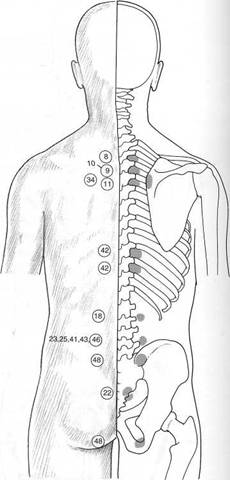
Fig. 4.15 Chapman’s neurolymphatic reflexes.
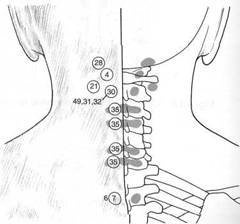
Fig. 4.16 Chapman’s neurolymphatic reflexes.
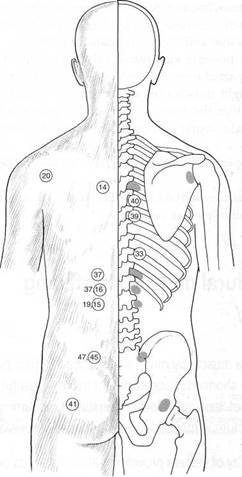
Fig. 4.17 Chapman’s neurolymphatic reflexes.
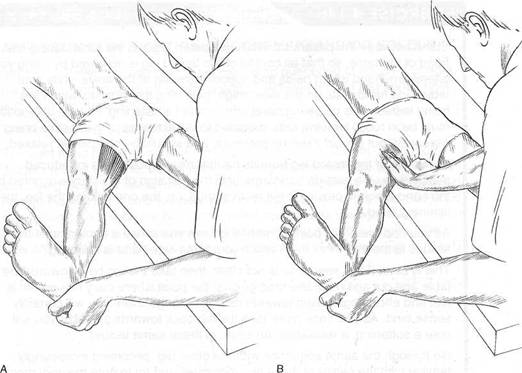
Fig. 4.18 Assessment of ‘blind’/restriction barrier with the first sign of resistance in the adductors (medial hamstrings) of the right leg. (A) The operator’s perception of the transition point, where easy movement alters to demand some degree of effort, is regarded as the barrier. (B) The barrier is identified when the palpating hand notes a sense of bind in tissues which were relaxed (at ease) up to that point.

Fig. 4.19A Assessment of gastrocnemius and soleus. The sole of the foot should achieve a vertical position without effort once slack is taken out via traction on the heel.
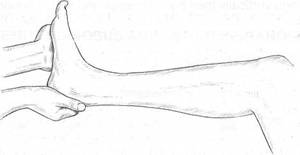
Fig. 4.19B With the knee flexed, the same assessment is evaluating the status of soleus alone.

Fig. 4.20 In the test position, if the thigh is elevated (i.e. not parallel with the table) probable psoas shortness is indicated. The inability of the lower leg to hang more or less vertically towards the floor indicates probable rectus femoris shortness (TFL shortness can produce a similar effect).
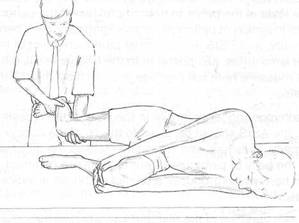
Fig. 4.21 Assessment for shortness of TFL – modified Ober’s test. When the hand supporting the flexed knees is removed the thigh should fall to the table if TFL is not short.
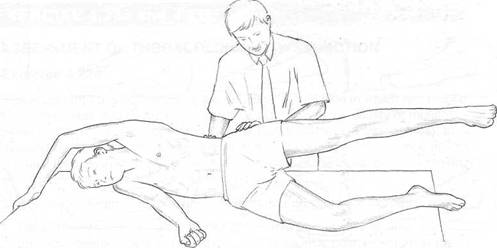
Яд. 4.22 Palpation assessment forquadratuslumborum overactM/, The musc/e /spa/pateC/, as is (he gfufeus medi’us, during abduction of the leg. The correct firing sequence should be jluteus, followed at around 25° elevation by quadratus. If there is an immediate ‘grabbing’ action )y quadratus it indicates overactivity, and therefore stress, so shortness can be assumed.
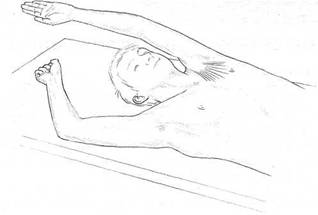
Fig. 4.24 Assessment of shortness in pectoralis major and latissimus dorsi. Visual assessment is used: if the arm on the tested side is unable to rest along its full length, shortness of pectoralis major is probable; if there is obvious deviation of the elbow laterally, probable latissimus shortening is indicated.
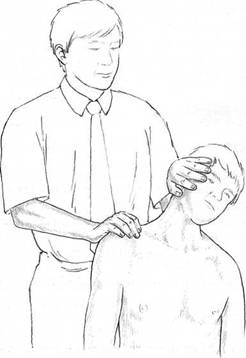
Fig. 4.25 Assessment of relative shortness of right side upper trapezius. The right shoulder is stabilised while the neck is side-bent to its first sign of resistance (‘bind’)without force. One side is compared to the other. Normal range is thought to be approximately 45°.